For most women in this age group, routine imaging isn't automatically recommended unless you have specific risk factors. But your forties can bring real shifts - hormonally, cardiovascular, and beyond - and for some women, targeted screening can make a meaningful difference.
This page outlines the imaging options that may be worth discussing with your GP or specialist, depending on your personal history and risk profile. A referral is generally required for any imaging.
Please note: These are imaging-based pathways available within our private radiology setting. They are in addition to, and do not replace other screening programmes offered through Health New Zealand.
Screening options
Low-dose CT (LDCT) is a safe, quick scan that can detect lung cancer at an early stage - when treatment options are broader, and outcomes are significantly better.
If you are a current or former smoker with a history of 20 pack-years or more, annual LDCT is worth considering, even if you feel completely well and have no symptoms. The scan requires no injections or sedation, and uses less radiation than a standard CT.
What makes LDCT particularly valuable is its ability to find lung cancer before symptoms develop - which is precisely when it's most treatable. For anyone at increased risk, it offers a proactive and straightforward way to keep a closer eye on lung health, and to act early if anything needs attention.
Cardiovascular disease often develops without any obvious warning signs - and for some, risk can be higher than they realise, even if they feel perfectly well. You may be at increased risk if you have one or more of the following:
- Diabetes, which increases inflammation and can speed up artery damage
- A family history of early heart disease
- High blood pressure or high cholesterol
- A history of smoking
- Long-term stress, low activity levels, or excess weight
- Age - particularly from 50 onwards
In individuals with these risk factors, cardiovascular disease can develop earlier and progress more quickly, and symptoms may be subtle or absent until later stages.
A CT Calcium Score is a specialised scan that detects calcium deposits in the arteries supplying your heart - a direct sign of plaque buildup that can narrow or block blood flow, raising your risk of coronary artery disease, angina, or heart attack. Importantly, it can find this before any symptoms appear, giving you and your care team time to act.
What makes it particularly useful is that it gives a concrete picture of what's actually happening in your arteries, rather than estimating risk based on lifestyle factors alone. From around age 50, a CT Calcium Score is worth discussing with your doctor or cardiologist as part of understanding and managing your cardiovascular health.
If you are a known BRCA gene carrier or have a similar elevated risk, 6–12 monthly transvaginal pelvic ultrasound may be recommended as part of your ongoing care.
A pelvic ultrasound is gentle, radiation-free, and well-suited to regular monitoring over time. As part of a surveillance programme, it can help pick up subtle changes early - when options tend to be simpler - or offer reassurance when everything looks normal.
It's worth knowing that in people with a higher genetic risk, changes can sometimes appear earlier or behave differently than in the general population, which is why regular monitoring can make a real difference.
Ultrasound works best as part of a wider care plan - alongside genetic counselling, specialist review, and any other tests your doctor recommends. Think of it as one of several tools working together, each adding a different layer of understanding to your overall picture.
If you have a known genetic mutation or a significant family history, it's worth asking your doctor whether 6–12 monthly ultrasound monitoring is right for you.
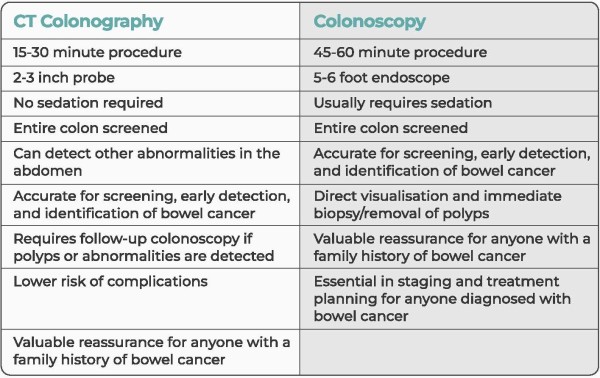
CT Colonography is a safe, effective, and considerably more comfortable alternative to traditional colonoscopy for bowel cancer screening - with no sedation required, a quicker procedure, and a faster recovery.
In New Zealand, access to conventional colonoscopy can be limited, meaning wait times are often long. CT Colonography offers a timely and reliable alternative, helping more women access bowel screening without unnecessary delay.
For women at low risk, CT Colonography every five years is a sensible way to screen for bowel cancer and other changes to the colon and rectum - typically beginning around age 50. If you are at higher risk - due to family history of bowel cancer, previous polyps, or other risk factors - you may benefit from starting screening earlier, and we recommend discussing with your doctor whether beginning screening in your 40s may be appropriate.
Bowel cancer is highly treatable when caught early, which is exactly what regular screening is designed to do.
CT Colonography is a fast, accurate, and less invasive alternative to colonoscopy. See the comparison below for more information.
You may have heard that WB-MR is able to ‘check for everything’ and find disease early. While it can be used for screening or early detection in some situations it is not a complete test for all diseases, and it's important to understand its limitations.
Currently there is no evidence to demonstrate significant improvement to your health outcomes using whole‑body MRI as a screening tool. It can also identify incidental or low‑risk findings that may lead to unnecessary anxiety and follow‑up tests. In addition to this, not all diseases are detectable on whole‑body MRI - particularly in the early stages - which can offer you false reassurance.
Whole-body MRI may be appropriate:
- As part of specialist-led care or surveillance
- In high-risk genetic conditions such as Li-Fraumeni Syndrome (inherited TP53 loss)
- For specific medical reasons, such as inflammatory or systemic disease
We recommend screening that is targeted, and evidence based, matched to your own risk profile, and using imaging that’s known to improve outcomes (such as bowel, lung and the other screening options defined above).
If you believe a whole-body MRI may be appropriate for you, please discuss the potential benefits, limitations, and suitability of the test with your doctor and arrange a referral to book your appointment with us.
For women in their 40’s, screening recommendations vary based on your personal risk profile.
It's important to discuss this with your healthcare provider and have your risk assessed. From there you can consider the options that best suit your profile and arrange a referral.
Please note, the recommendations below sit alongside, build upon, and are separate from BreastScreen Aotearoa, the national screening programme which offers free mammograms every two years.
Tomosynthesis
Tomosynthesis (also known as 3D mammography) captures multiple images from different angles, allowing the breast to be viewed in thin layers rather than a single flat image. This reduces the overlap of normal tissue, making it easier to identify small or subtle abnormalities that might otherwise be hidden - offering greater confidence in the results over standard mammography.
Annual tomosynthesis is recommended for women in this age group.
Contrast Enhanced Mammography
Contrast Enhanced Mammography (CEM) is a specialised mammogram that uses a small amount of contrast dye to highlight areas of increased blood supply in the breast. This can help detect cancers more clearly - particularly in dense breast tissue - by showing changes that may not be visible on standard mammography or tomosynthesis alone.
For women with denser breasts (BIRADS C or D) or a moderate to high risk profile, CEM is recommended every second year. By alternating with routine screening, it provides an additional layer of sensitivity and improves the chance of detecting cancers earlier.
MRI Breast
For women with denser breasts (BIRADS C or D) or a moderate to high risk profile, MRI may also be recommended periodically alongside annual tomosynthesis - or as an alternative to CEM. MRI uses a different technology, without radiation, that is more sensitive than mammography, making it better placed to pick up small or early abnormalities that may be difficult to see even with tomosynthesis.